
PALS Megacode Scenarios: The 2025 AHA Standards Every Healthcare Provider Needs to Know
PALS MEGACODE SCENARIOS
The 2025 AHA Standards Every Healthcare Provider Needs to Know
By Finish Strong CPR & Medical Training

Pediatric emergencies are unforgiving. A child in cardiac arrest or respiratory failure gives you seconds — not minutes — to make the right call. That’s exactly why the American Heart Association’s Pediatric Advanced Life Support (PALS) program exists, and why mastering the megacode scenarios at the heart of PALS certification is non-negotiable for every healthcare provider who works with children.
The 2025 AHA standards bring important updates to pediatric resuscitation — from refined weight-based dosing protocols to clearer decision trees for respiratory distress vs. failure vs. arrest. Whether you’re renewing your PALS certification or preparing for your first course, this guide walks you through the core megacode scenarios, what evaluators are looking for, and how the 2025 guidelines change the way you respond.
What Is a PALS Megacode — and Why Does It Matter?
A PALS megacode is a simulated, high-stakes pediatric emergency scenario used during certification testing. Unlike written exams or isolated skill stations, a megacode tests your ability to lead a resuscitation team, recognize deterioration, integrate algorithms in real time, and communicate clearly under pressure — simultaneously.
You’ll be assessed as the team leader. That means you’re not just performing skills; you’re directing your team, calling for medications, interpreting rhythm strips, reassessing the patient after every intervention, and making time-critical decisions out loud.
Passing isn’t about perfection. It’s about demonstrating that you have a systematic approach, you know when to escalate, and your team is moving in the right direction.
The 2025 AHA Updates You Need to Know
The AHA’s 2020 guidelines were a significant reset for pediatric resuscitation, and the 2025 updates build on that foundation with refinements backed by the latest evidence. Key changes affecting megacode performance include:
High-quality CPR standards remain the anchor. The 2025 guidelines continue to emphasize push hard, push fast — compression depth of at least one-third the anterior-posterior diameter of the chest (approximately 2 inches for most children, 1.5 inches for infants), rate of 100–120/min, full chest recoil, and minimized interruptions targeting a CPR fraction above 80%.
Epinephrine timing is reinforced. For non-shockable rhythms (PEA and asystole), give epinephrine as soon as IV/IO access is established — every 3–5 minutes thereafter. Don’t let rhythm checks or team transitions delay the first dose.
Ventilation during CPR. For intubated pediatric patients, the 2025 standard is one breath every 2–3 seconds (20–30 breaths/min), asynchronous with compressions. For non-intubated patients, the 15:2 compression-to-ventilation ratio remains the standard for two-rescuer pediatric CPR.
Post-resuscitation care starts in the room. The 2025 standards place greater emphasis on targeted temperature management, avoiding hyperthermia after ROSC, and initiating a post-cardiac arrest care bundle before the patient leaves your care area.
The Core PALS Megacode Scenarios
The AHA structures PALS megacodes around two primary arrest pathways and a set of pre-arrest recognition scenarios. Here’s what you need to know about each.
Scenario 1: Respiratory Distress Progressing to Failure
| THE SETUP
An 8-year-old with a history of asthma presents with increased work of breathing, nasal flaring, intercostal retractions, SpO₂ of 88% on room air, and a respiratory rate of 38. He is anxious and unable to speak in full sentences. |
What the evaluator is watching for
The primary objective here is recognition and intervention before respiratory failure becomes respiratory arrest. The cascade goes fast in children — once a child fatigues, they decompensate quickly.
Your first move is oxygen. High-flow O₂ via non-rebreather mask while you assess. You should be simultaneously calling for a bag-mask device and positioning the child upright.
In a known asthmatic, the cause is lower airway obstruction. Albuterol via nebulizer or MDI with spacer is first-line. Ipratropium adds anticholinergic bronchodilation. Systemic corticosteroids should be given early — their onset is delayed, so earlier is always better.
If SpO₂ doesn’t improve, be ready to escalate to CPAP or positive pressure ventilation with BVM. The moment you start assisting respirations, your team needs to know.
| Key PALS Principle: Respiratory failure is the most common pathway to pediatric cardiac arrest. Treat aggressively before the child tires. |
Scenario 2: Shock — Recognition and Management
| THE SETUP
A 3-year-old girl presents after 3 days of vomiting and diarrhea. She is lethargic, HR 172, BP 72/40, capillary refill 4 seconds, extremities cool and mottled, absent radial pulses with a weak central pulse. |
What the evaluator is watching for
This scenario tests your ability to classify shock and execute the correct fluid and vasopressor strategy. The 2025 AHA standard for pediatric shock resuscitation is 20 mL/kg IV/IO isotonic fluid bolus, reassessing after each bolus.
Shock classification determines your path:
- Hypovolemic: fluids are your primary treatment
- Distributive (septic): fluids + vasopressors if fluid-refractory (epinephrine or dopamine)
- Cardiogenic: conservative fluid (5–10 mL/kg), vasopressors early, cardiology involvement
- Obstructive: treat the underlying cause immediately — fluids alone will not fix this
| Key PALS Principle: Compensated shock has a pulse and a blood pressure. Decompensated shock is the emergency. Know the difference — and treat compensated shock aggressively before it decompensates. |
Scenario 3: Pulseless Arrest — VF / Pulseless VT (Shockable)
| THE SETUP
A 10-year-old athlete collapses during practice. He is unresponsive, apneic, and pulseless. The monitor shows coarse ventricular fibrillation. |
What the evaluator is watching for
The algorithm is shock-first. Deliver a single defibrillation at 2 J/kg for the first shock. After the shock, immediately resume CPR for 2 minutes before checking rhythm. Do not delay CPR to “see if it worked.”
After 2 minutes, check rhythm. If still VF/pVT, increase to 4 J/kg for subsequent shocks. Epinephrine 0.01 mg/kg IV/IO enters after the second shock, every 3–5 minutes. Amiodarone (5 mg/kg) or lidocaine (1 mg/kg) for shock-refractory VF/pVT after the third shock.
Search for reversible causes — the H’s and T’s — at every rhythm check. In a young athlete, consider hypertrophic cardiomyopathy, long QT syndrome, commotio cordis, and electrolyte abnormalities.
| Key PALS Principle: Shock first, then CPR — immediately. Every second of delay to defibrillation reduces survival. Minimizing CPR interruptions is equally non-negotiable. |
Scenario 4: Pulseless Arrest — Asystole / PEA (Non-Shockable)
| THE SETUP
A 6-month-old infant is brought in by EMS. Parents found her unresponsive in her crib. She is apneic, pulseless, and the monitor shows a flat line. |
What the evaluator is watching for
Non-shockable arrest in a child is almost always preceded by respiratory failure or shock. The algorithm is CPR + epinephrine. Start CPR immediately — two-thumb encircling technique for infants is the preferred 2-rescuer method per 2025 AHA standards.
Establish IV/IO access and give epinephrine 0.01 mg/kg as soon as access is secured. Repeat every 3–5 minutes. There is no role for defibrillation in asystole or PEA — delivering a shock to a non-shockable rhythm is a critical error that will fail your megacode.
The H’s and T’s are your roadmap — verbalize your search during the megacode:
| The H’s | The T’s |
| Hypoxia | Tension pneumothorax |
| Hypovolemia | Tamponade (cardiac) |
| Hydrogen ion (acidosis) | Toxins |
| Hypo/Hyperkalemia | Thrombosis (pulmonary) |
| Hypothermia | Thrombosis (coronary) |
| Key PALS Principle: In non-shockable pediatric arrest, CPR quality and early epinephrine are your only tools. Maximize both. Find and fix the reversible cause. |
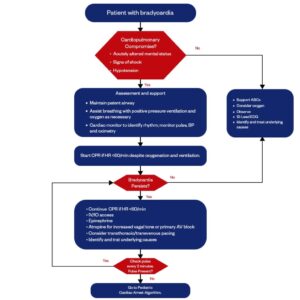
Scenario 5: Bradycardia with a Pulse and Poor Perfusion
| THE SETUP
A 2-year-old with a HR of 54, low blood pressure, altered mental status, and poor perfusion. Known history of a congenital heart defect. |
What the evaluator is watching for
First, support oxygenation and ventilation. Hypoxia is the most common cause of bradycardia in children. Give high-flow O₂. If the rate doesn’t improve with oxygenation, move to medications.
- Epinephrine (0.01 mg/kg IV/IO) — first-line for symptomatic bradycardia not responding to oxygenation
- Atropine (0.02 mg/kg IV/IO, minimum 0.1 mg) — indicated for increased vagal tone or primary AV block
- Transcutaneous pacing — if medications fail and the child is deteriorating; verbalize this in your megacode
| Key PALS Principle: Treat the child, not just the number. Bradycardia with good perfusion needs monitoring. Bradycardia with poor perfusion needs intervention — now. |
What PALS Megacode Evaluators Are Really Grading
Beyond algorithm adherence, evaluators are assessing your leadership and communication. The most common reasons providers fail a PALS megacode have nothing to do with forgetting a drug dose.
- Closed-loop communication is mandatory. When you give an order, your team member must repeat it back and confirm execution.
- Verbalize your thinking. Evaluators cannot read your mind. Say what you see. Thinking out loud is not a weakness — it’s leadership.
- Manage the resuscitation, don’t participate in it. As team leader, step back, watch the whole patient, and direct your team.
- Reassess after every intervention. Every medication, every fluid bolus, every shock — you must reassess and verbalize what you find.
Preparing for Your PALS Megacode: A 5-Step Framework
- Know your weight-based dosing cold. Use the Broselow tape during the scenario — but practice your calculations so you’re not starting from zero under pressure.
- Run the algorithms out loud. Don’t just read the algorithm cards. Verbalize them. Your mouth is slower than your brain — the real scenario will feel faster.
- Practice team leadership separately from clinical skills. Most providers over-rehearse the clinical steps and under-rehearse the leadership.
- Know your H’s and T’s reflexively. In every arrest scenario, be able to run through all ten reversible causes in under 30 seconds.
- Debrief every practice run. A 10-minute debrief after each simulation builds more competency than three additional run-throughs without reflection.
PALS certification isn’t a box to check. It’s a commitment to every child and family who will one day depend on you in their worst moment. The 2025 AHA standards represent our best current evidence for what works. Learn them. Practice them. Own them.
| Ready to certify or recertify your team?
Finish Strong CPR & Medical Training offers on-site PALS and ACLS courses with scenario-based instruction aligned to the latest 2025 AHA standards. “Confident Teams. Compliant Workplaces.” |
Tags: PALS · Pediatric Advanced Life Support · AHA 2025 · Megacode · Pediatric Resuscitation · CPR Certification · Finish Strong CPR


